Prepared by Chris Kolb, Ph.D.
Vice-Chair, Jefferson County Board of Education
Tuesday, January 26, 2021
Introduction
As an elected body, the Jefferson County Board of Education is subject to open meetings laws, meaning that the board must conduct any substantial discussion in public. To abide by these laws, I would normally wait until the next school board meeting to communicate with my colleagues. However, COVID-19 is so consequential to the welfare of our community that I believe it would be negligent to delay, and so I am releasing a public statement.
At the school board meeting on January 19, I presented a significant amount of research regarding the safety of returning to competitive winter sports given the current state of the pandemic. I have updated this information below. In addition, I am concerned that some of my colleagues expect teachers and other JCPS employees to return to in-person work before it is safe to do so. I have also included information addressing this.
As I wrote in early September, no one in JCPS is under any illusion that NTI is as effective as in-person instruction. With NTI, we are doing our absolute best in an unprecedented situation that has already killed over 400,000 Americans and will kill tens of thousands more. NTI has been very difficult for my own fourth-grader and for my family as a whole, so I know first-hand how challenging NTI is for kids and parents. My kid wants to go back to school in-person very badly. The pandemic has had noticeable negative effects on him. I deeply understand the frustrations families have because I experience all the same frustrations.
I recognize that not being in school in-person has negative effects on children and families. However, many of those negative effects — for instance, economic hardship due to lost parental work time — are problems that other governmental entities are failing to address. School systems are used to taking on ancillary responsibilities to make up for inaction at other levels of government, but there is a limit to what school systems can do. JCPS cannot return to in-person learning to solve problems that other decision-makers have ignored.
For the reasons outlined below, I am inclined to support NTI only until everyone in the community has had the opportunity to be vaccinated, until the positive test rate is five percent or less for two weeks, or until Jefferson County is in the “orange” for two weeks and cases in Louisville are steady or declining.
The Current COVID-19 Situation
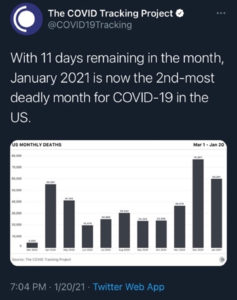
While trends are beginning to show some positive movement, the pandemic has been worse than ever in recent days, both nationally and locally. As The Washington Post reported, “On [Nov. 3, 2020], the U.S. had never had a day with more than 100,000 new cases; since Nov. 5, it has never had a day with fewer than that.” As a result, January will be the deadliest month in the U.S. by far (figure 1).
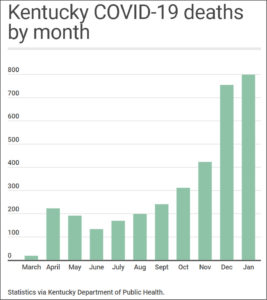
On September 30, Gov. Andy Beshear stated that the 1,018 cases reported that day should serve as a “wake-up call,” and he warned Kentuckians that “We can’t let this thing get out of control again because we’re tired.” Kentucky failed to heed this warning, as on January 6 alone the state reported 5,447 new cases, over five times the amount that Beshear regarded as a wake-up call. On September 6, Gov. Beshear announced that Kentucky had set a record for the number of weekly cases, with 4,742, and he stated that “We’re facing the challenge of our lifetimes and we must do better.” We did not do better, as between January 14 and 20 Kentucky reported over 20,000 new cases. As a result, Kentucky set a new record for deaths in a month with six days still to go in January (figure 2).
Local trends largely mirror statewide data. Louisville recently broke a record for new cases in a week, leading Chief Health Strategist Dr. Sarah Moyer to conclude that “We have entered into another surge.” Since the pandemic began, the test positivity rate in Louisville has never been lower than 7.4 percent, and in recent days it has hovered between 13 and 17 percent (figure 3).

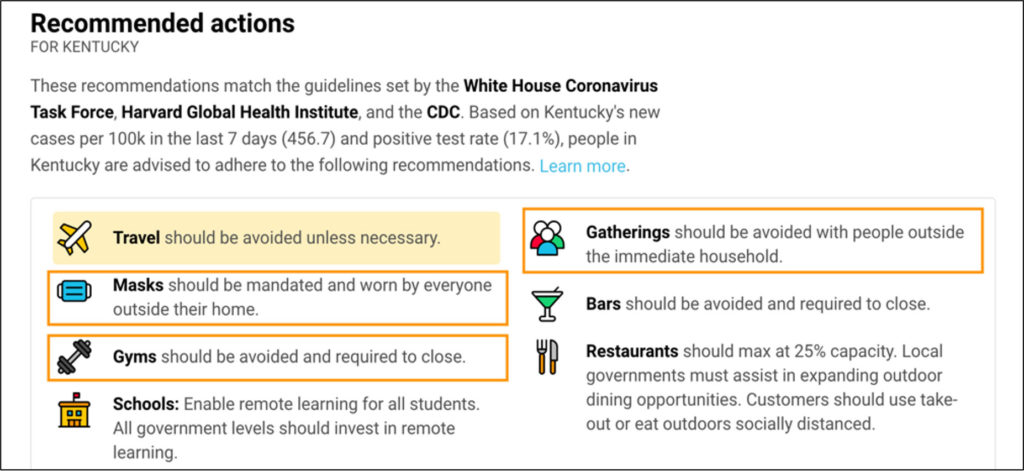
The Johns Hopkins School of Public Health states that: “As a rule of thumb … one threshold for the percent positive being ‘too high’ is 5 percent. For example, the World Health Organization recommended in May that the percent positive remain below 5 percent for at least two weeks before governments consider reopening. … A high percent positive means … it is not a good time to relax restrictions [and] … it may be a good time to add restrictions.” Given the current situation, these are recommended actions for Louisville (figure 4).
Sports and COVID-19
The local positivity rate alone is enough to warrant suspending most sports in a competitive setting. However, several other indicators also support this conclusion. The Center for Disease Control and Prevention lists 13 risk factors that should be assessed when deciding if sports are appropriate. The majority of these factors indicate that it is not advisable to play competitive winter sports at the moment (figures 5, 6, 7, 8, & 9).
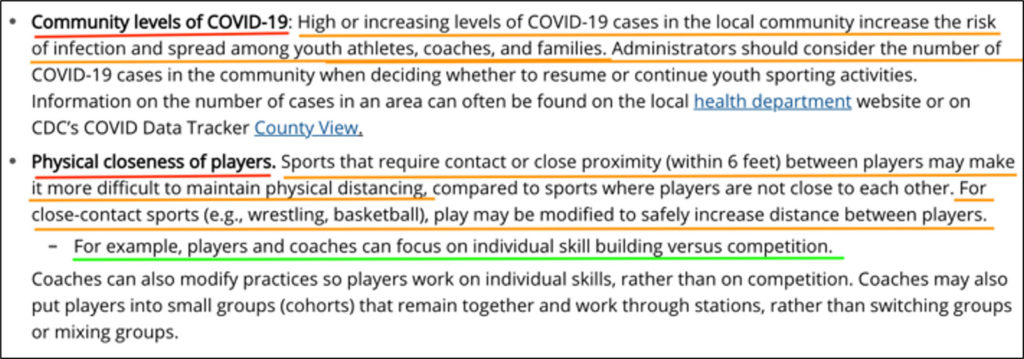
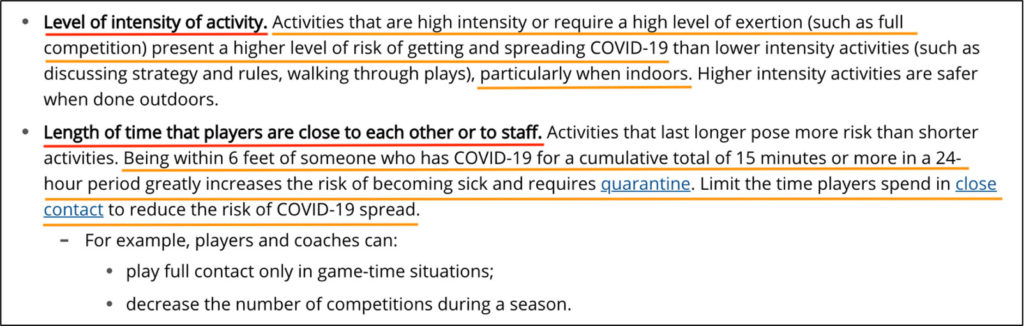
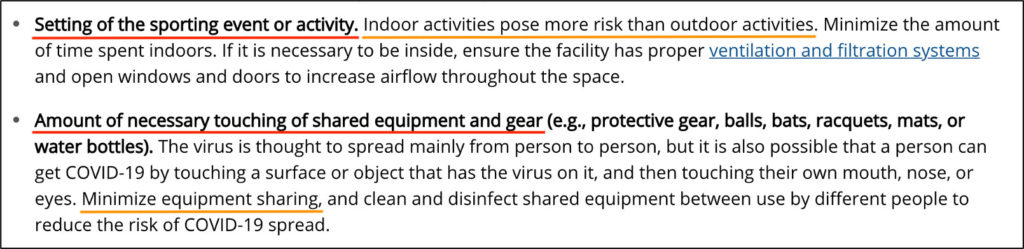
Of particular relevance locally, the CDC advises decision-makers to consider the number of players who have a higher risk of developing severe illness, such as those with asthma (figure 8). According to the Asthma and Allergy Foundation of America, Louisville is the seventh worst metropolitan area in the U.S. for asthma (figure 9).


Further increasing the risk of winter sports is that CDC research indicates that people with no symptoms spread almost 60 percent of all cases of COVID-19. This means that, short of rapidly testing everyone who may participate in or attend a sporting event, even the most stringent and rigorous procedures will fail to identify over half of all people who are positive for the virus. As one medical expert put it: “Many people won’t know they’re contagious based on their symptoms, which may be encouraging them to go about their daily lives with a false sense of safety. … These findings suggest that just identifying and isolating people who have symptoms isn’t enough to control the ongoing spread of the coronavirus. It doesn’t catch all the cases.”
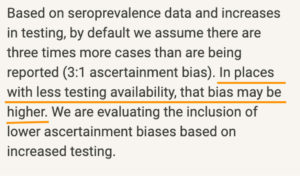
The Georgia Tech COVID-19 Event Risk Assessment Planning Tool gives further cause for concern. Due to insufficient testing in Louisville, researchers at Georgia Tech advise that there are at least five times as many COVID-19 cases in Louisville as are being reported (figure 10). Using an “ascertainment bias” of five with a crowd of only 100 people yields a 97 percent chance that at least one person in the crowd will be COVID-19 positive (figure 11).
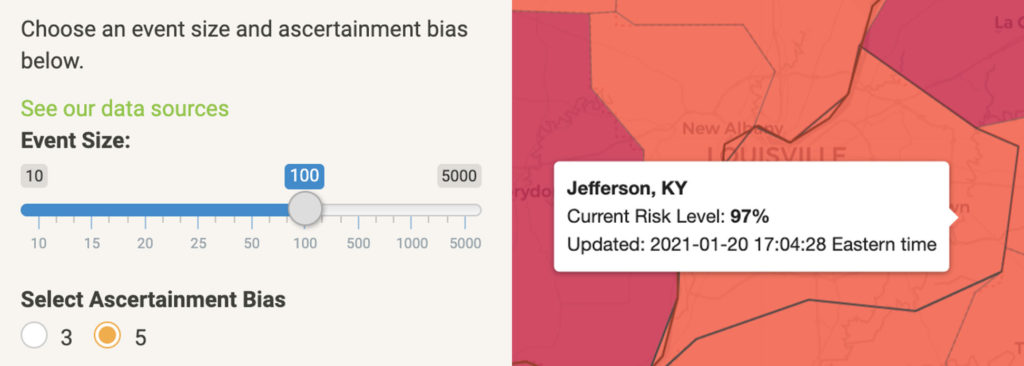
JCPS is planning to allow 225 or more people to participate in or attend basketball games. Thus, if a crowd of 100 yields a 97 percent chance that at least one person will be positive — and a 58 percent chance at least one person will be positive and asymptomatic — then more than doubling the crowd to 225 will make it a virtual certainty that more than one person at such an event will be positive for COVID-19, and at least one person will be asymptomatic, making them prime candidates to spread the virus. This is especially true if one of them is a coach, referee, or athlete, who will be yelling and breathing inches away from other people’s faces.
Why Vaccination Alone Is Not Enough
While the development and distribution of a vaccine is tremendously hopeful news, several facts indicate that, on its own, vaccinating K-12 school personnel will not be enough to foster a safe return to in-person education or many competitive sports.
Most importantly, while vaccination may lessen the rate of transmission, it is likely that many people who are vaccinated will still transmit the virus. Thankfully, their symptoms will probably be mild or non-existent. However, by transmitting the virus to people who have not yet been vaccinated, they will put unvaccinated individuals at risk, including members of their families. Moreover, vaccinations are not yet approved for those under 16 years old, meaning that children will still spread the virus to others, including unvaccinated members of their families. Finally, vaccination is about 95 percent effective, meaning that “one out of every 20 people who get this vaccine could still get moderate to severe infection.”
In addition, there is evidence that more contagious strains of the virus are now spreading, and, “infectious disease specialists are concerned that any strain that is more contagious … might quickly increase the number of COVID-19 cases.” Thus, the CDC advises that “Experts need to understand more about the protection that COVID-19 vaccines provide before deciding to change recommendations on steps everyone should take to slow the spread of the virus.” In other words, the vaccine has not yet caused the CDC to change guidance about schools or sports. If state officials decided to vaccinate K-12 personnel with the expectation that we should move away from this guidance, then they were not listening to the CDC.
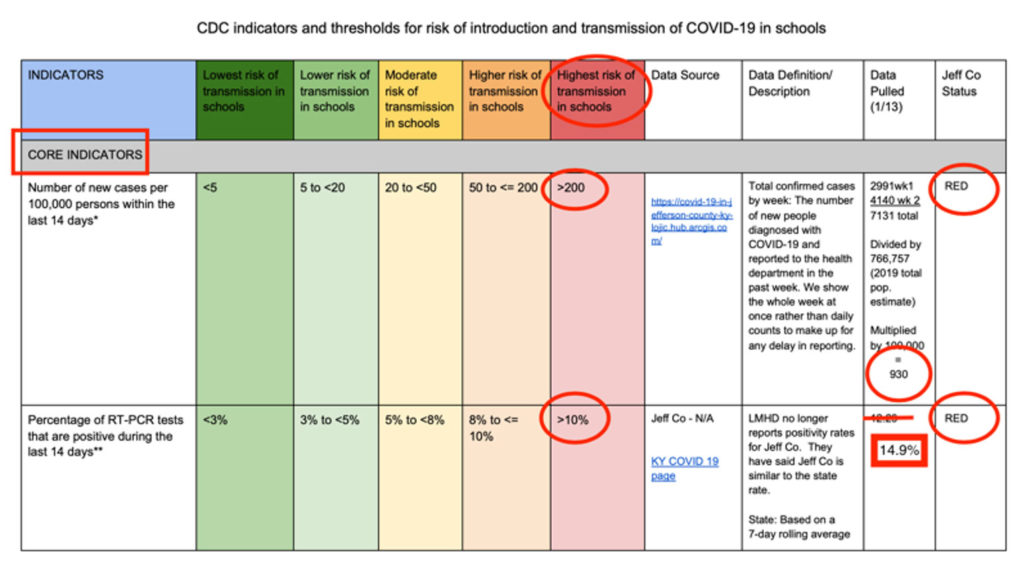
According to the core indicators the CDC encourages school districts to use in determining whether in-person instruction is advisable, recent data indicates that Louisville significantly exceeds the thresholds for even the highest-risk category. On Jan. 14, Louisville had almost five times the number of new cases needed to meet the criteria for “highest risk,” putting Louisville in quintuple red territory (figure 12). In addition, for some time the positivity rate has hovered between 25 and 50 percent higher than the threshold for highest risk (figures 3 and 12). Phase one vaccinations in Kentucky are not expected to conclude until the summer, when phase two vaccinations (for anyone over 40) are only expected to begin. Thus, up until the traditional end of the school year in late May there will be many people over the age of 60, many people with health risks, and many essential workers who will not yet be vaccinated.
Finally, there is evidence that returning to in-person instruction leads to higher rates of community transmission of COVID-19. “After preying heavily on the elderly in the spring, the coronavirus is increasingly infecting American children and teens in a trend authorities say appears fueled by school reopenings and the resumption of sports, playdates and other activities.” Moreover, some studies indicate that children are, “twice as likely to pass on the virus than adults.” This is even more concerning given that new strains of the virus appear to be more contagious. Thus, “Because these new strains are more contagious, a lower level of community spread may put in-person schools at risk of an outbreak,” making the high positivity rate in Louisville even more concerning.
In short, even after K-12 school personnel have all been vaccinated, the community transmission rate is likely to remain the best indicator of the danger that the virus poses. This conclusion is supported by recent research that indicates, “in-person … options are not associated with increased spread of COVID at low levels of pre-existing COVID cases, but cases do increase at moderate to high pre-existing COVID rates.” Thus, absent a significant decline in community transmission, competitive winter sports and in-person school will contribute to a higher rate of community transmission, which will lead to increased illness, hospitalization, and death in these groups. While all K-12 school personnel could be vaccinated by the end of March, many of their children, partners, and extended family members will not be. In my view, it is unwise to ask teachers and other staff to choose between risking the lives of their family members and keeping their jobs, especially given the growing teacher shortage.
Practical Considerations
Practical concerns also make a return to in-person school problematic. Here is how one JCPS teacher sums many of them up: “I am concerned about the loss of instructional time if we return. We will be spending weeks on teaching expectations. If we return before spring break, that time will be used to teach expectations and then we will have to re-teach expectations when returning from spring break. These are weeks that could be used to teach content if we were to continue with NTI for this school year. … Speaking for my class, my students are set on their very structured schedule they have for NTI and know exactly what to expect and are comfortable with their current routine. Is there really a benefit in changing this on our students for 10 or less weeks?”
Moreover, transportation remains an unsolvable dilemma. While many parents will decide to continue NTI if we return to school in-person, an unknown number of buses will still transport a higher number of students than can be distanced from one another. In fact, JCPS may still transport three students to a seat on buses. Invariably, some number of students on these buses will contract COVID in the community. In confirmed cases, this will mean quarantining many people from a bus. More concerning, however, is that many cases will not be diagnosed, making buses a rich environment for COVID transmission given the limited spacing available.
In addition, as there is no natural link between teachers who will return to an in-person setting and students who will do so, a large percentage of students will not have the same teacher they have had for more than half of the school year. Students may not even have a teacher who worked at their school prior to returning to in-person instruction. While this is unavoidable if we return to in-person school, this is a regrettable outcome that could have an extremely negative affect on student learning, student belonging, and school culture overall.
Direct Risks to Children
While COVID-19 does not make children as sick as it does adults, and while children only rarely suffer serious complications like Multisystem Inflammatory Syndrome, this does not mean that risks to children are negligible. For example, a recent study by the Children’s Hospital of Philadelphia found that all children who had COVID-19, including those who never had any symptoms, showed signs of blood vessel damage. In most children this included, “clotting in the small blood vessels [that] has been identified as a potential cause for severe manifestations of COVID-19 in adults.”
In addition, myocarditis (inflammation within the heart) is a risk for everyone, including children, and can be especially dangerous for athletes. As one doctor for Big Ten athletes put it, “What we have seen is when people have been studied with cardiac MRI scans — symptomatic and asymptomatic COVID infections — is a level of inflammation in cardiac muscle that just is alarming.” This led Dr. Stephen Stack, Commissioner of the Kentucky Department for Public Health, to ask: “How comfortable are we all allowing sports to happen, not knowing if [myocarditis] is going to be as big a problem as the early signal suggested? How many high school parents, if their child plays sports and is diagnosed with COVID-19, how many parents can afford to pay for an electrocardiogram, blood draws, and an echocardiogram?”
Finally, there are indications that, like serious illnesses in the past that are similar to COVID-19, the virus may lead to long-term neurological damage. “Strokes have occurred in COVID-19 patients of all ages — and in fact, physicians have reported that some adults under 50 have presented to the hospital with strokes as their first complication from COVID-19.”
In sum, I believe Dr. Stack identified a core issue when he stated, “We don’t want to experiment with our kids if we don’t know what the consequences will be.” However, this is exactly what we are doing by returning to competitive sports, and what we will be doing if we return to in-person instruction while the pandemic is still raging in Louisville.
The Weakness of Counterarguments
My school board colleagues have argued that it is not fair that our students are some of the only people in our city and our state being asked to sacrifice for the greater good. There are two weaknesses to this argument.
First, our students are not the only ones sacrificing. By taking actions that will increase the rate of community transmission, JCPS is asking the following groups to increase their sacrifice:
- healthcare workers like nurses, nursing assistants, and employees of long-term care facilities, one of whom I suggest you read about here;
- essential workers, many of whom go to work for low wages so we can all continue to buy food, gas, and whatever we want from retailers;
- people over 60 (higher risk);
- people who are pregnant (higher risk);
- people with common medical conditions like asthma, diabetes, obesity, high blood pressure, heart disease, and cancer (higher risk);
- the 95,000+ JCPS students who are not athletes — including many of the 12,000+ ECE students — who are now less likely to be able to return to in-person school;
- healthy younger people who are unlucky enough to experience severe symptoms — like the so-called “long-haulers” — including death.
By returning to competitive athletics and potentially returning to in-person education, we are forcing tens of thousands of Louisvillians in these categories to risk their health and, potentially, to sacrifice their lives. Thousands of JCPS students, parents, grandparents, and employees are in these categories. However, school board members are elected by the whole community, and thus we are charged with promoting the overall community well-being, including the interests of those with no direct ties to JCPS.
The second weakness of this argument is that those who make it are attempting to absolve themselves of responsibility for consequences of their decision by claiming that the decisions of others leave them no choice. Surely, I’m not the only one whose mother continually admonished them that it would be unwise to jump off a bridge just because someone else did. In the end, those who make this argument are arguing that we should capitulate to peer pressure and simply do it because others are doing it.
My colleagues have also argued that students from more well-off families are able to play sports with private clubs while student from poorer families are not. This is surely true. However, the cause of equity is not furthered by exposing the most vulnerable populations to higher risk of infection and serious complications. As the Louisville Department of Public Health and Wellness states: “The Black community, other communities of color, communities experiencing poverty, and others are more heavily burdened by chronic illness. These chronic illnesses are also risk factors for experiencing severe COVID-19 complications, and lead to high death rates among those communities.”
Thus, if JCPS makes a decision that leads to more infections, our actions will have an especially negative impact on people in these groups. On top of this, many of our students in these communities live with older caretakers who are at much greater risk. As a result, students from already challenging environments are more likely to lose their family members and caretakers, and many of their families will take on mountains of medical debt that come with prolonged hospital stays and lifelong health problems.
One of my colleagues has also indicated that JCPS should return to in-person instruction after school personnel are vaccinated because the state and city “are moving heaven and earth” so JCPS employees can be vaccinated. This is inaccurate. State and city governments are working to vaccinate as many people as possible because it is their job to do so. I hope we have not come to expect so little of our elected leaders that performing basic governmental functions is seen as a special favor to the citizens who elect them.
Conclusion
As one constituent wrote to me: “Since the start of this horrific pandemic, JCPS has always stated that the number one priority is the health and safety of staff and students. I can confidently say that I felt that it was during the fall, but I feel that health and safety is slowly slipping to the second or third spot.” By deciding to return to winter sports competition on January 19, JCPS can no longer say that health and safety is our top priority.
As a non-partisan board of education, we have a particular responsibility to make decisions based on facts, evidence, and data, and not on politics, public pressure, personal biases, concern for re-election, or any other factor. As always, I am open to changing my conclusions based on new evidence and data or based upon evidence and data I have not yet reviewed. The current evidence and data, however, lead me to the conclusion that it is simply not safe, wise, or responsible to return to competitive winter sports or in-person instruction until everyone in the community has had the opportunity to be vaccinated, until the positive test rate is five percent or less for two weeks, or until Jefferson County is in the “orange” for two weeks and cases in Louisville are steady or declining.
Unfortunately, the community has not committed itself to doing what is required to make in-person education possible. As Norton Healthcare Infectious Diseases and System Epidemiologist Dr. Paul Schulz stated: “‘There’s a significant percentage of the population that has not altered their behavior.’ … That’s what it all goes back to, people deciding what’s essential and what’s not in protecting their own health and the health of others.” Until the community decides that in-person education is more essential than other things like bars and restaurants being open for indoor service, JCPS faces a steep uphill climb in returning to in-person instruction.
Recommended Resources
Considerations for Youth Sports Administrators, Center for Disease Control and Prevention.
COVID-19 in Jefferson County, KY, Louisville Metro Department of Health and Wellness.
COVID-19 Dashboard, Kentucky Department for Public Health.
COVID-19 Event Risk Assessment Planning Tool, Georgia Tech University.
COVID Act Now Kentucky and Louisville dashboards. (See here for info about COVID Act Now.)
Indicators and Thresholds for Risk of Introduction and Transmission of COVID-19 in Schools, Center for Disease Control and Prevention.
Tracking the Spread of the Coronavirus Outbreak in the U.S., Bloomberg News.